The Connection Between Ankle Mobility & Squat Depth
As a fitness professional, you’ve likely encountered clients who struggle to achieve full depth in their squats. While many focus on hip or knee flexibility, restricted ankle dorsiflexion is often an overlooked factor.
In fact, ankle mobility plays a critical role in squat mechanics, and improving this range of motion can make a significant difference in both depth and overall form.
This can also be seen on the reformer in Pilates and in the yoga studio with difficulty getting into certain positions such as chair pose.
The Anatomy Behind Ankle Dorsiflexion
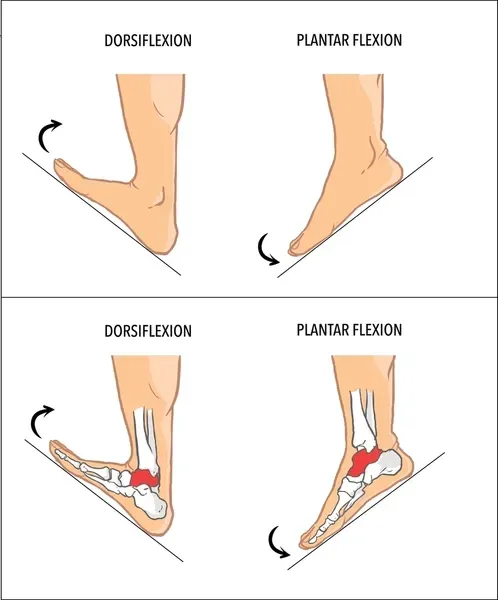
Ankle dorsiflexion refers to the ability to bring the top of the foot closer to the shin, a movement controlled by muscles such as the tibialis anterior (responsible for pulling the foot upwards).
However, this motion can be restricted by tight structures like the gastrocnemius and soleus muscles, both of which form the calf and insert into the Achilles tendon, which then inserts into the calcaneus.
The average, functional range of ankle dorsiflexion is approximately 15-20 degrees. If your clients lack this degree of movement, they are likely to compensate in their squat by shifting their weight forward, lifting their heels off the ground or collapsing their feet, resulting in poor mechanics and increased injury risk.

Why This Matters to You as a Fitness Professional
1. Improved Squat Mechanics:
During a squat, the knee travels forward over the toes to maintain balance and depth. If the ankle cannot dorsiflex properly (at least 15-20 degrees), the knee will be restricted, causing compensations like:
Forward torso lean: To maintain balance, the client leans forward, putting excessive strain on the lower back.
Heels lifting off the ground: This alters stability and shifts weight distribution, reducing the efficiency of the squat.
Foot rolling inwards: This causes the knees and hips to roll in.
2. Injury Prevention:
Limited dorsiflexion leads to compensatory movement patterns, such as knee valgus (knees caving in) or excessive hip hinging. Over time, these poor mechanics can cause stress on the joints, particularly the knees, hips, and lower back, leading to overuse injuries.
Unlocking a Client's Squat Potential
Let’s say you have a client who struggles to achieve deep squats despite having good hip and knee mobility. They frequently lean forward or round their lower back at the bottom of the squat.
After assessing their ankle dorsiflexion using the knee-to-wall test (where the knee should reach the wall with the foot 6-8cm away), you discover they have less than 10 degrees of dorsiflexion. This lack of mobility in their ankles is forcing them to compensate elsewhere in the body.
By incorporating calf stretches, dynamic ankle mobility drills (like wall-assisted dorsiflexion stretches or ankle rocks), and targeted strengthening exercises for the lower leg muscles, you help them gradually restore full ankle range of motion.
Over time, they achieve deeper, more stable squats with better knee tracking, reducing the strain on their lower back and knees.
Actionable Tips for Improving Ankle Mobility
1. Ankle Mobility Drills
Wall-Assisted Dorsiflexion Stretch: Have the client place their foot flat on the ground with the knee bent towards the wall. Hold for 20-30 seconds to target the soleus and improve ankle range of motion.
Ankle Rocks: While kneeling or in a half-kneeling position, push the knee forward over the foot forwards and backwardsin a rocking motion, moving through the ankle joint to promote increased dorsiflexion. Perform 10-15 reps per side. A theraband loop can be added - fixed from behind you and around the ankle, below the malleoli, essentially gliding the talus posteriorly to assist this motion.
Try This Simple Theraband Assisted Ankle Dorsiflexion Drill.
2. Calf Stretching and Flexibility
Straight-Leg Calf Stretch: Target the gastrocnemius by placing the hands against a wall and stepping one foot back. Keep the heel on the ground and the back knee straight while leaning forward. Hold for 30 seconds.
Bent-Knee Calf Stretch: Shift focus to the soleus by performing the same stretch with a bent knee. This allows deeper penetration into the deeper calf muscles, which often limit dorsiflexion.
Try This Simple Gastrocnemius With Arch Lifted Stretch
3. Self-Myofascial Release
Foam Rolling the Calves: Have your client roll their calves using a foam roller or massage ball. Encourage them to roll from just above the ankle to the back of the knee, stopping to apply pressure on any tight or tender spots for 20-30 seconds.
Integrating Ankle Mobility into Your Programs
To effectively address ankle mobility without disrupting your client’s overall training program, integrate these drills into their warm-ups or active recovery sessions.
You’ll find that even dedicating just a few minutes to ankle mobility can make a significant difference in squat performance and help prevent compensations that may lead to injury.
In my online course, I provide in-depth assessment techniques for ankle mobility and corrective exercises designed to enhance your client’s movement patterns.
By focusing on mobility from the ground up, you can help your clients achieve their full strength potential in exercises like squats, deadlifts, and lunges.
Click here to unlock your clients’ full squat potential by prioritising ankle health!
